PocketAnatomy® is a registered brand name owned by © eMedia Interactive Ltd, 2009-2022.
iPhone, iPad, iPad Pro and Mac are trademarks of Apple Inc., registered in the U.S. and other countries. App Store is a service mark of Apple Inc.

Anatomy Thumb side, further row of carpal bones, between scaphoid and 1st metacarpal, has deep palmar groove for flexor carpi radialis. Attachments; origin opponens pollicis, and abductor, flexor pollicis brevis, transverse carpal ligament. The saddle-shaped surface articulating with 1st meta-carpal allows large range of thumb movement including opposition. Clinical Often removed in treatment of basal
- Published in Pocket Anatomy Pins

Anatomy Above 2nd metacarpal in further row of carpal bones, wedge-shaped, narrow end palmar. Articulates up with scaphoid, down with 2nd metacarpal, in with capitate, out with trapezium. Least injured carpal bone. Clinical “Sam Likes To Play; Try To Catch Him”. S, L, T, P, proximal row; T, T, C, H; distal row, lateral (thumb)
- Published in Pocket Anatomy Pins
.jpg)
Anatomy Origin: Lateral head: Posterior surface of the humerus superior to the radial groove. Long head: Infraglenoid tubercle of the scapula. Medial head: Posterior surface of the humerus inferior to the radial groove. Insertion: Olecranon process of the ulna and deep fascia of the forearm. Key Relations: -Long head lies between teres minor and teres
- Published in Pocket Anatomy Pins
.jpg)
Anatomy Origin: Long head: Infraglenoid tubercle of the scapula. Lateral head: Posterior surface of the humerus superior to the radial groove. Medial head: Posterior surface of the humerus inferior to the radial groove. Insertion: Olecranon process of the ulna and deep fascia of the forearm. Key Relations: -Long head lies between teres minor and teres
- Published in Pocket Anatomy Pins
.jpg)
Anatomy Origin: Medial head: Posterior surface of the humerus inferior to the radial groove. Lateral head: Posterior surface of the humerus superior to the radial groove. Long head: Infraglenoid tubercle of the scapula. Insertion: Olecranon process of the ulna and deep fascia of the forearm. Key Relations: -Medial heads lies posterior to the long and
- Published in Pocket Anatomy Pins

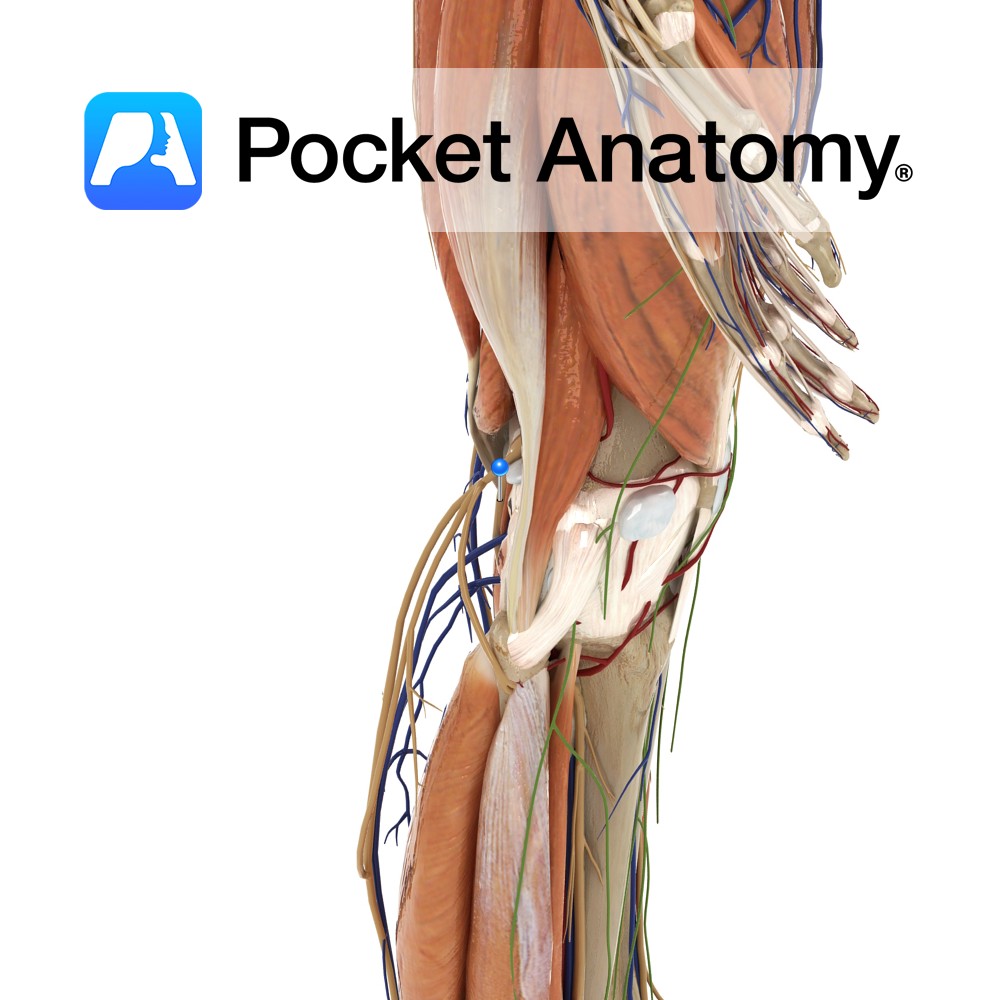
Anatomy Large long bulge front of upper shaft, where patellar ligament (ie central part of common tendon of quadriceps femoris; rectus femoris, vastus medialis, intermedius and lateralis). Clinical The tuberosity has an apophysis and fractures can occur in active adolescents. Osgood-Schlatter disease/syndrome is an associated, usually self-limiting painful condition affecting active children 9-16 (boys 5:1
- Published in Pocket Anatomy Pins
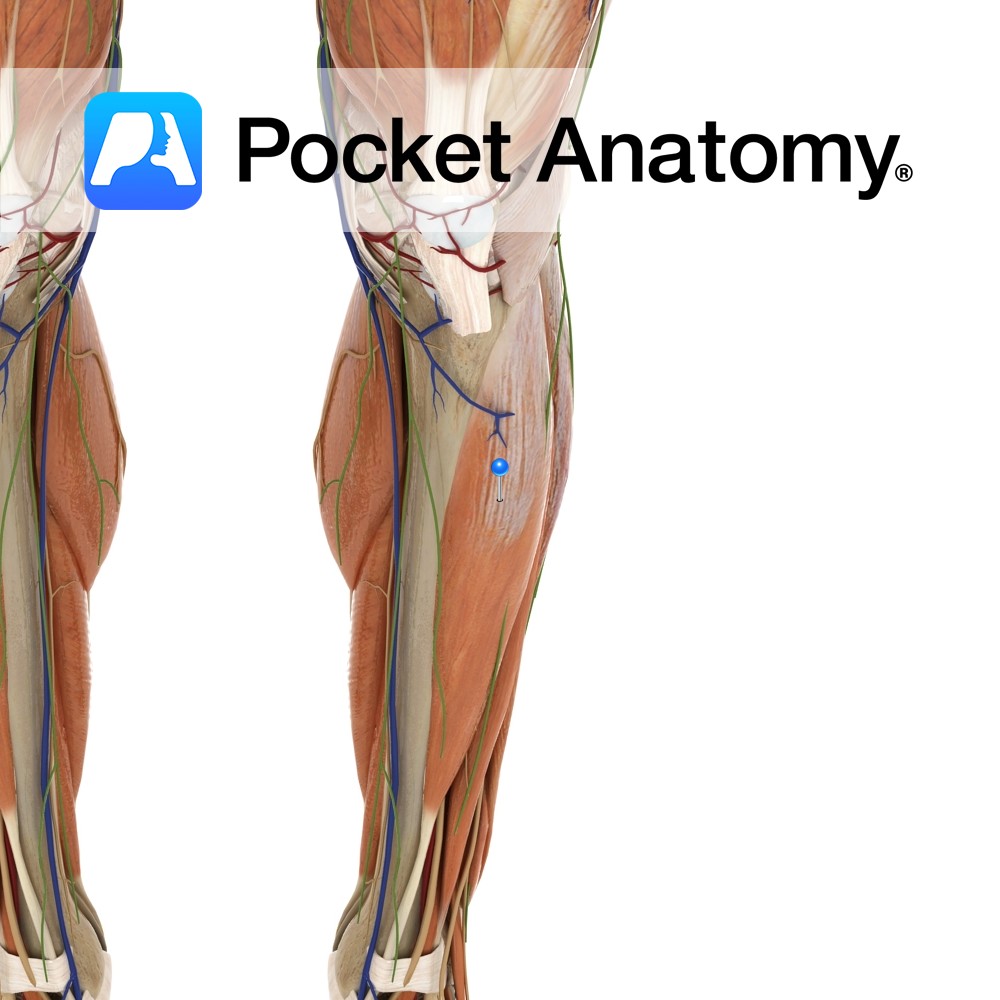
Anatomy Course A terminal branch of the sciatic nerve, and so contains fibres from the spinal segments of L4 – S3. The sciatic nerve becomes the tibial nerve upon exiting the popliteal fossa. It passes under the tendinous arch formed by the soleus muscle and descends in the plane between the solus and the tibialis
- Published in Pocket Anatomy Pins
Anatomy Origin: Inferior surface of the lateral condyle and upper two-thirds of lateral surface of the tibia and the interosseous membrane. Insertion: Medial surface of the medial cuneiform and the base of 1st metatarsal. Key Relations: -One of the four muscles of the anterior compartment of the leg. -The tibialis anterior tendon crosses anterior to
- Published in Pocket Anatomy Pins
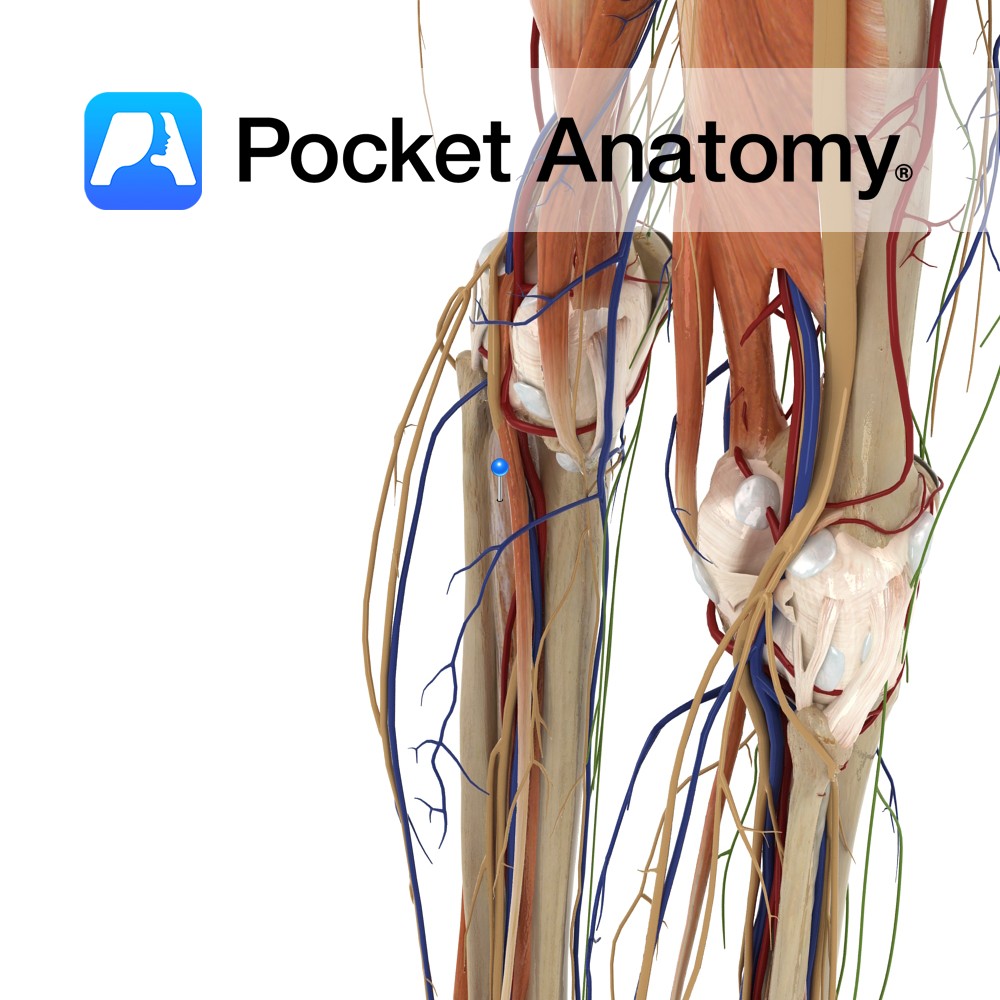
Anatomy Origin: Posterior surfaces of the tibia below the soleal line, posterior surface of the fibula and posterior surface of the interosseous membrane. Insertion: Tuberosity of the navicular, all cuneiforms, cuboid and the bases of the 2nd, 3rd and 4th metatarsals. Key Relations: -One of the four muscles of the deep posterior compartment of the
- Published in Pocket Anatomy Pins
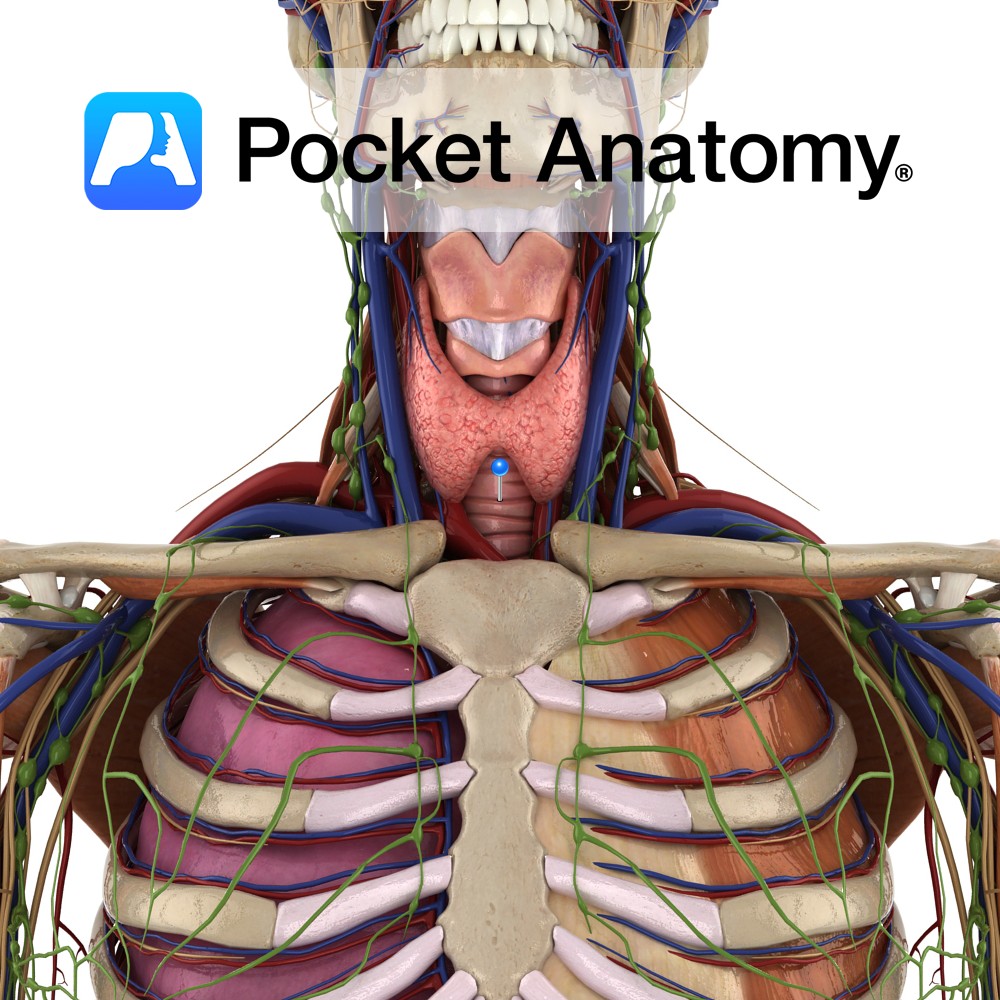
Anatomy Windpipe, anterior of neck in front of esophagus, connects larynx (at level C6) and lungs (epiglottis in larynx closes, protects lungs against swallowed material from pharynx); c. 4″ long, 1″ diameter; splits into right/left bronchi level T5; epithelial lining with cilia and mucus provides part of conditioning of inspired air, trapped material wafted up,
- Published in Pocket Anatomy Pins