Anatomy
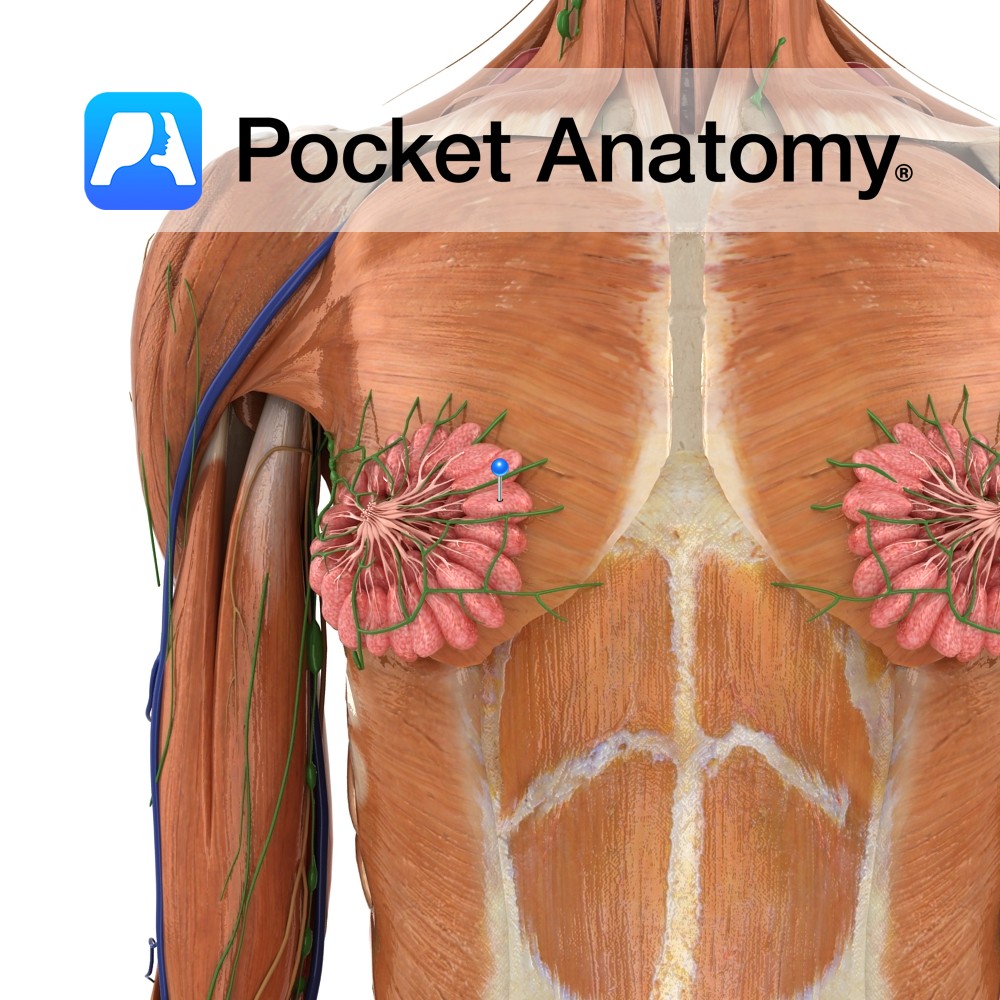
Paired skin-covered mammary (milk-producing) gland (modified apocrine/sweat gland) ventral (in front of) pectoralis major muscle on thoracic/chest wall, levels ribs #2 to 6; can extend to axilla at side (sometimes as far as latissimus dorsi at back), up to clavicle, in/medial to sternum, made of adipose/glandular/connective/myoepithelial tissue, comprising 15-20 irregular lobes (each with 10-100 secretory acini/sacs in clusters/alveoli) opening into milk, then larger lactiferous ducts (lumens 2-4mm diameter) which converge on and open to exterior at nipple. Ligaments (Cooper’s) and connective tissue suspend the breast. Lymphatic drainage 75% to ipsilateral (same side) axillary nodes, 25% to abdominal nodes and o other side.
Areola are circular (can be elliptical) pigmented area around breast, variable size, bigger after puberty, bigger/darker (average diameter 1.5″, persisting) after pregnancy/lactation, occasional hair, 5 – 20 Montgomery’s tubercles (as small bumps/protrusions) – openings of sebaceous glands (radially situated around nipple).
Areolar (Montgomery’s) glands are sebaceous, 5-30 each breast, under nipple and areola, developing at puberty, opening onto them as/at raised Montgomery’s tubercles (in a ring around and also on nipple), secreting lubricant when stimulated (sexual or rooting), under influence oxytocin.
Physiology
Develops at puberty under influence of estrogen, changes each month as part of menstrual cycle (water retention), size further increases during pregnancy under influence estrogen/progesterone/prolactin (tissue ratio glandular:fat 1:1 non-lactating, 2:1 lactating), glandular tissue shrinks/disappears post-menopause (with gradual/variable accompanying ptosis/sag). Lactation/emptying (following stimulation of nipple/areola) influenced by oxytocin (there is a muscular/contractile element, as myoepithelial cells surround acini). Erogenous zone (particularly nipple/areola), stimulation pleasurable. Breast changes size/weight/shape/texture under hormonal influences of estrogen/progesterone/prolactin/oxytocin at childhood/puberty/menstruation/pregnancy/lactation/menopause. Breast size not an indicator of ability to breastfeed.
Areola darkens during pregnancy. Colour may be a factor in assisting rooting baby.
Areolar gland secretion is mainly lipoid (oily, not watersoluble) fluid, protecting nipple, possibly olfactory component also attracts/guides rooting baby, higher incidence cracking/infection when disturbed/disrupted.
Clinical
Breast cancer common, usually arising from ducts/lobules, 1% male 99% female, accounts for >20% of female cancers and 70% 5-year survival in developed countries, early detection possible through screening mammography though benefits controversial, treatment depends on type/stage and includes surgery/chemotherapy/radiotherapy/hormonotherapy/immunotherapy, mortality % and 5-year survival %. Exercise, alcohol moderation, non-smoking, breastfeeding reduce risk.
Areolar glands develop at puberty, prominent in pregnancy/lactation, ducts occasionally join with lactiferous such that milk appears at tubercle. Can block, swell, develop cyst.
Paget’s disease (cancer), otherwise non-symptomatic, may come to attention as eczematous nipple/areola.
Interested in taking our award-winning Pocket Anatomy app for a test drive?
![]()